AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-1897/050
Assistant Professor, Department of General Surgery, Government Medical College, Nagpur, Maharashtra, India
*Corresponding Author: Dr. Kamatham Aashish, Assistant Professor, Department of General Surgery, Government Medical College, Nagpur, Maharashtra, India. Dr. Sanjay S Changole Associate Professor, Department of General Surgery, Government Medical College, Nagpur, Maharashtra, In
Citation: Paul T E Cusack Multiple Sclerosis J. Surgi Case Rep and Imag. 4(1). Doi: 10.31579/2690-1897/050
Copyright: © 2021 Paul T E Cusack, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 October 2020 | Accepted: 11 November 2020 | Published: 02 January 2021
Keywords: Trauma, geriatric patients, road traffic accidents, Injury severity score, mortality
India is the second-most populous country in the world has about 76.6 million people at or over the age of 60, constituting above 7.7% of total population. A cross-sectional study of 300 cases of geriatric and non-geriatric population groups was conducted at well-established Trauma, Orthopaedic and Neurosurgical services centre in Central India. Mechanisms of injury sustained by the participants showed that Falls which include both Ground level falls (GLF) and Fall from height (>2 metres) contributed to 55.4% cases in the geriatric population. The next most common cause of trauma in the geriatric population was road traffic accidents amounting to 34.3% of the cases. Data on the injuries sustained by both the study cohorts in terms of the different body regions based on Abbreviated Injury Scale (AIS) and Injury severity score (ISS) showed the head region was most consistently and maximally injured in both the study populations. Comorbidity profiles of geriatric and non-geriatric trauma populations showed significantly high hypertension, cerebrovascular disease, diabetes, diminished hearing and vision among the geriatric group. The maximum number of geriatric patients underwent Orthopaedic and spine surgeries (44.9%), Intercostal drain placements (34.6%), while the non-geriatric population had a higher number of Craniotomies (40%) and Intercostal drain placement (33.5%) surgeries respectively. The geriatric population had a significantly higher crude mortality rate of 39.3% compared to the non-geriatric population ( 26.3% ). With reference to intervention procedures, the geriatric population had a lower percentage of operative intervention and a higher rate of conservative management as compared to the non-geriatric population.
Worldwide people are living longer with increased life expectancy. In the world's population, the aged and older population of age 60 years and above is expected to cross over by 2.1 billion by 2050. According to the WHO, 80% of all older people will live in low- and middle-income countries by 2050 [1] According to the State of World Population 2019 report by the United Nations Population Fund (UNFPA), released last week, India's population in 2019 stood at 1.36 billion, growing from 942.2 million in 1994 and six percent of India's population was of the age 65 and above [2]. Currently, patients older than 65 years account for 23% of all trauma admissions, and trauma represents the fifth leading cause of death in this population. In view of the high prevalence of multiple comorbidities in the elderly, there is an increased likelihood of death or severe disability following trauma [3,4,5]. The risk of death after trauma is significantly increased in patients older than 65 years of age, and for those over the age of 80, it is approximately four-fold that of younger patients. Further, the economic costs, as well as the societal cost are higher following trauma to elderly patients. Thus, the social and economic implications are expected to increase in geriatric trauma and clinicians must continue to strive toward a more standardized and evidence-based approach to the diagnosis and treatment of these patients.
The effect of age as a predictor of mortality in older adult trauma is difficult to assess from the existing published literature. Traditional trauma protocols have been established and proven in the treatment of younger accident victims. Older people with diminished physiological reserve, often in association with significant co-morbidities, require special consideration. The distribution of injuries and the type of injury mechanism is likely to be different in a population with a high incidence of osteoporosis [6]. Older patients can become multiply injured following low energy trauma and these injuries may have worse outcomes [7]. Patients with limited mental or physical capacity are more likely to be involved in accidents as they are slower to identify and respond to dangerous situations. Medical emergencies such as myocardial infarction or stroke precipitating an accident, making it necessary to treat this pathology alongside the patient's injuries. Mental and physical incapacity can make an assessment of these patients troublesome. Older patients may become confused and uncooperative during comparatively minor physiological derangements, often compromising their investigation or treatment [8, 9]. For these reasons, it is important to accurately document the pattern of injuries and clinical course of older patients with severe injuries. Recent reports of polytrauma in older adults are limited and the subject has previously been given only brief attention. This study aims to identify and characterize the geriatric population with poly-trauma and compare them to non-geriatric trauma patients in terms of severity of injuries, patterns of injury patterns, mortality and comorbidities trauma exposed to various mechanisms of injury and trauma.
2.1 Study Setting: The study was conducted at a tertiary and well-established trauma care centre in Central India with Orthopaedic care, Trauma and Neurosurgical services. It is a well established hospital in these three specialties.
2.2 Study population: All geriatric and non-geriatric patients who had been admitted in the Trauma Care Centre through emergency medical services from June 2017- November 2019, who met the inclusion criteria were monitored in the trauma care centre until death/discharge in the wards were included in this study.
2.3 Inclusion criteria: Patients consenting to participate. Adult trauma patients from ages 18 – 64 years were admitted to the Surgical Casualty and Trauma Care Centre. Adult trauma patients from ages 65 – 89 years were admitted to the Surgical Casualty and Trauma Care Centre.
2.4. Exclusion criteria: Patients with penetrating traumatic injuries – gunshot and stab wounds. Patients below 18 years and above 90 years.
2.5. Sample size: The sample size is calculated as: Power (1-beta)%: 80%; Alpha error %: 5. Minimum sample required in each group n = 116 (Geriatric and Non-geriatric)
2.6. Estimated final sample size: 300 cases each in both geriatric and non-geriatric population groups were enrolled in this study in accordance with the inclusion criteria.
2.7. Sampling Method: Study participants were drawn from all the patients who were admitted to the tertiary trauma centres of central India from June 2017 to November 2019. All adult trauma admissions from ages (18 –89 years) were subjected to the pre-determined inclusion criteria. Participants were then subsequently divided into two cohorts from all eligible adult trauma patients - the first consisting of a control group of all patients ages 18 to 64 years (non-geriatric patients) and the second consisting of all patients ages 65 to 89 years (geriatric patients). The included study subjects were then examined in accordance with the various parameters included in the proforma below.
2.8. Variables collected for each group were
Admission demographics.
Vital signs and physiological parameters on admission.
Mechanism of injury subdivided into falls (with a subgroup of ground level falls and falls from height (<2>
The primary outcome was the type of injuries sustained and injuries were divided by ICD-9 code into the following categories:
2.9. Research instruments
Pre-tested proforma was used to collect information bedside after clinical examination and by going through the patient charts. One research assistant accomplished by filling the admitting part of the questionnaire at casualty and confirmed by the author.
2.10. Data collection management and analysis
Data collection was done through a structured proforma as described above at the Emergency Department and in the ward. After admission, these patients were monitored until death/discharge and the relevant data was entered accordingly. This was done with assistance by pre-trained admitting staff and assisted by other doctors in the ward. The filled proforma were examined and the data was then systematically compiled in a master sheet using Microsoft Excel Program. All the variables and parameters were then subjected to statistical analysis.
2.11. Statistical Analysis
The data were analysed using PASW 18.0 Software; formerly known as SPSS 18.0 Software. The statistical analysis for comparative assessment will include, use of Student's t-test (for continuous scale data) and Pearson's ChiSquare test with Yates correction for categorical variables. Logistic regression analysis was also carried out to identify those factors independently affecting a certain outcome.
2.12. Ethical consideration
Permission to carry out the study was granted by MUHS research ethical committee. Additionally, informed consent was requested from the participants In line with consent, participants have explained the nature and purpose of the study.
The results obtained from a comparative cross sectional study conducted on injury and trauma, mortality, morbidity in geriatric and non-geriatric patients admitted in a tertiary care trauma centre in central India is outlined below. The demographic profile of the participants in relation to the age distribution showed a male sex preponderance in both the population groups. Among non-geriatric patients, 62.7% and 52.6% were male patients, 37.3% and 47% were female patients respectively among geriatric and non-geriatric trauma patients. The geriatric population group showed a clear male preponderance with males making up 62.7% of the study group.
The age distribution in the geriatric population group affected by injury and trauma ranged from 65-89 years. The maximum number of fatalities occurred in 65-69 age group while the 85-89 year remains the least affected. Mean age from this study cohort was 72 years. The age distribution in the non-geriatric study population ranged from 18 to 65 years. The age group of 18-27 years had the maximum number of fatality cases with the mean age in the non-geriatric cohort was found to be 39 years.
Vital parameters such as mean systolic and diastolic blood pressure, mean pulse rate and the number of patients with a Glasgow Coma Score were recorded in both the study (Table 1). These parameters represent the baseline vital signs with which both the populations present to the trauma care centre. Further, these parameters signify the derangements in the physiology secondary to the traumatic event in both populations.
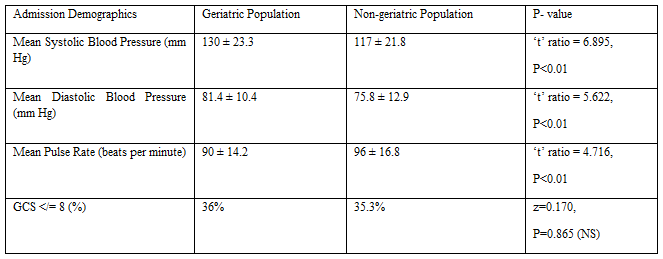
The geriatric trauma population had a higher mean systolic blood pressure (130 mm Hg) compared to the non-geriatric counterparts who showed a mean of (117 mm Hg). Similarly, the mean diastolic blood pressure in the geriatric age group was relatively higher in the non-geriatric population. The mean pulse rate in the geriatric group was lower compared to the non-geriatric group with a mean of 90 ±14.2 and 96 ±16.8 bpm respectively. Glasgow Coma Scale (GCS) is a neurological scale that aims to give a reliable and objective method of recording the state of a person's consciousness for initial as well as subsequent assessment. A GCS of >/=8 is classified as severe brain injury. A shown in Table 1, 36% of patients showed GCS score <8 in both geriatric and non-geriatric patients.
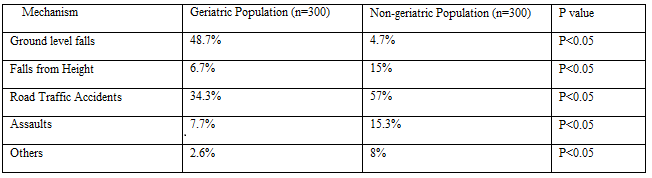
Mechanisms of injury sustained by the participants from both the cohorts i.e. geriatric and non-geriatric populations is presented in Table 2. It is evident that Falls which include both Ground level falls (GLF) and Fall from height (>2 metres) contributed to the largest number of cases in the geriatric population amounting to 55.4% cases out of all the cases. The next most common cause for trauma in the geriatric population was Road traffic accidents amounting to 34.3% of the cases. The non-geriatric population showcased a different trend wherein, road traffic accidents contributed to the highest number of cases of 171 (57%). In contrast, the ground level falls had the least number of cases of 14 (4.7%) in this study population. Falls (ground level falls + falls from height) contributed to 19.7% of all the causes in the non-geriatric population.
Data on the injuries sustained by both the study cohorts in terms of the different body regions are presented in Table 3. These different body regions have an individual abbreviated injury score. The highest AIS scores 3 out of the total 6 regions are squared and summed to give to consolidated Injury severity score (ISS). Thus, both the geriatric and non-geriatric study populations had comparable Injury Severity Scores of greater than or equal to 16 which signifies a severe overall injury. The head region was most consistently and maximally injured in both the study populations. AIS >/=3 is defined as a severe injury to the head.
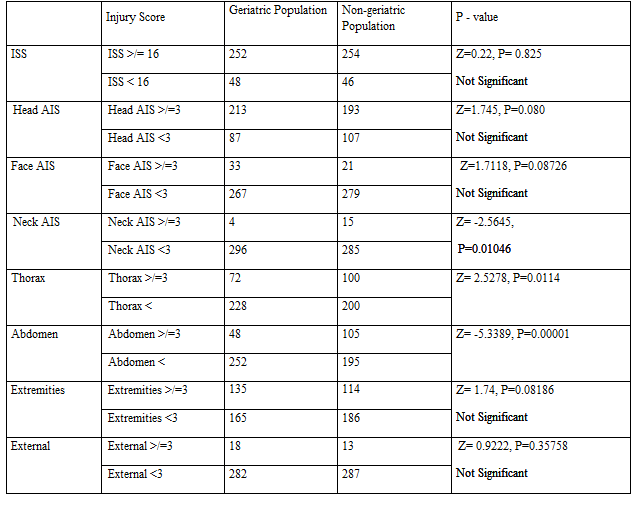
The non-geriatric cohort had AIS >/= 3 of head injury. The next highest contributor to morbidity in the non-geriatric cohort was also severe extremity injury with Extremity AIS >/=3. The non-geriatric population was observed to have sustained a much higher proportion of severe thoracic (100 vs 72) and abdominal injuries (105 vs 48) as compared to the geriatric counterparts, both of which were statistically significant.
Comorbidity profiles of geriatric and non-geriatric trauma populations are presented in Table 4. The geriatric study group had a significantly higher number of a wide range of comorbidities with many patients having more than 1 comorbidity simultaneously. Hypertension was the most common comorbidity noted amongst both the study groups although, the geriatric
study group had more than twice the number of cases with hypertension compared to the non-geriatric population i.e. 50% and 24% respectively. Cerebrovascular disease was noted amongst 25% and 17% of the geriatric and non-geriatric trauma populations respectively with the geriatric cohort showing a higher incidence. 27% of the geriatric study population was diabetic as compared to 24% of the non-geriatric population who also had diabetes mellitus. The diminished vision was noted in 30% of the geriatric trauma patients as opposed to just 13% of the non-geriatric patients having the same complaints. The diminished hearing was also primarily noted in the geriatric population with up to 28% of them having the above comorbidity as opposed to just 6% of the non-geriatric population having diminished vision.

Various injury patterns noted in both the study populations have been stratified by the various mechanisms of injury is presented in Table 5. Falls contributed to the highest number of cases (55%) in the geriatric population followed by RTA (34%) as the next major cause for trauma. Amongst the falls, Ground level fall has been the highest casualty at 87% as compared to fall from height (> 2metres) contributing 13% towards the total number of falls.

The head and extremities were most often injured in the geriatric population sustaining falls with 77% and 64% of them showing the above the two injuries respectively. The next major mechanism responsible for trauma in the geriatric age group is Road traffic accidents (RTA) with 34% of the population having sustained RTA. The head, extremities and thorax were once again most often injured at 72%, 48% and 35% respectively. In the non-geriatric population, RTA was the major cause of trauma responsible for 57% of the casualties with the head, extremities, thorax and abdominal injuries accounting for the injury patterns in the descending order.
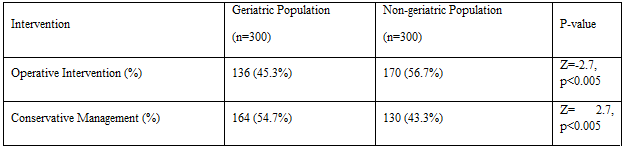
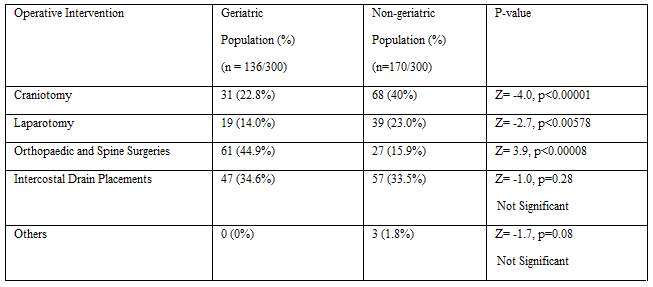
Table 6. Illustrates a comparison between the geriatric and non-geriatric trauma populations who underwent operative interventions and conservative management. It is evident that the geriatric population had a lower percentage of patients who underwent an operative intervention as compared to the non-geriatric population (45.3% vs 56.7%). Similarly, the geriatric population group had a higher rate of conservatively managed patients as compared to the non-geriatric population (54.7% vs 43.3%). Both the findings were statistically significant.
The different operative interventions underwent by the geriatric and non-geriatric trauma populations is presented in Table 7. The geriatric population had the maximum number of patients who underwent Orthopaedic and spine surgeries (44.9%) followed by Intercostal drain placements (34.6%), Craniotomies (22.8%) and Laparotomies (14%) in the decreasing order. The non-geriatric population had the maximum number of Craniotomies (40%) followed by Intercostal drain placements (33.5%), laparotomies (23%) and orthopedic and spinal surgeries (15.9%) in the descending order. It can be deduced that the geriatric population, even though had a high number of head injuries underwent a significantly fewer number of craniotomies compared to the non-geriatric population while a significantly higher number of orthopedic and spinal surgeries were performed in the geriatric age group as compared to the non-geriatric population. The non-geriatric population had a higher number of craniotomies performed as compared to the geriatric age group.
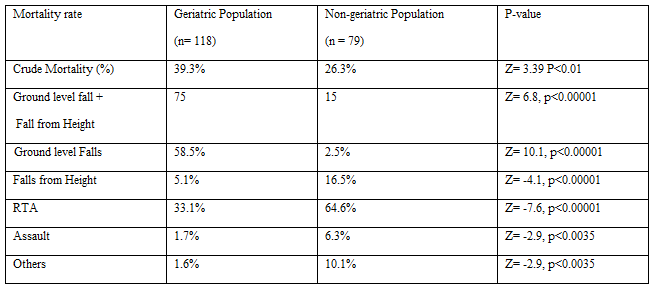
The geriatric population had a significantly higher crude mortality rate at 39.3% as compared to the non-geriatric population (Table 8). Falls especially ground level falls were responsible for the maximum number of mortalities (58.5%) among all mechanisms of injury followed by RTA (33.1%) in the geriatric trauma population. Road traffic accidents were the cause of the maximum number of mortalities (64.6%) amongst the non-geriatric population in the present study.
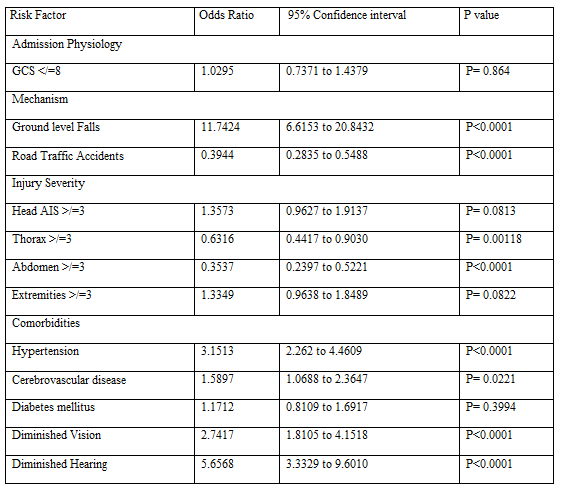
Factors that are independently associated with mortality for the entire population i.e. geriatric and non-geriatric populations is presented with statistical significance in Table 9. These factors have been identified on logistic regression analysis. Odds ratios are used to compare the relative odds of the occurrence of the outcome of interest (e.g. disease or disorder), given exposure to the variable of interest (e.g. health characteristic, aspect of medical history). The odds ratio can also be used to determine whether exposure is a risk factor for a particular outcome and to compare the magnitude of various risk factors for that outcome.
Odds ration=1 Exposure does not affect odds outcome.
Odds ratio >1 Exposure associated with higher odds outcome.
Odds ratio <1 Exposure associated with lower odds outcome.
It is clearly evident that Ground level falls (OR - 11.742 and CI - 6.6153 to 20.8432) are independently associated with mortality for the entire population and in the geriatric population ground level falls are significantly high compared to the non-geriatric group. Head (OR - 1.357 and CI - 0.9627 to 1.9137) and extremity injuries (OR - 1.3349 and CI - 0.9638 to 1.8489) are common in both population groups secondary to a traumatic event and thus, also independently are associated with mortality. Amongst, the comorbidities, it is clear that hypertension (OR - 3.1513 and CI - 2.262 to 4.4609), diminished vision (OR - 2.7417 and CI - 1.8105 to 4.1518) and diminished hearing (OR - 5.6568 and CI - 3.3329 to 9.6010) are other major contributors for mortality.
A comprehensive comparative cross-sectional study on mortality and morbidity and the factors affecting the trauma in geriatric and non-geriatric patients was conducted in a tertiary care and trauma centre in central India. An in-depth evaluation of comorbidities, mechanism of injury, injury pattern and preventive interventions in 300 geriatric population and non-geriatric trauma patients each were undertaken in this study after meeting the pre-decided inclusion criteria. These subjects were then evaluated according to the various parameters and the results obtained were subsequently analyzed.
Demographic details of both the cohorts were collected and analyzed. In our study, there was a significant male preponderance (62.7%) in the geriatric whereas the non-geriatric population showed a marginal increase in the males over the females. In the geriatric trauma population, there was a clear male predilection in every age distribution group. A retrospective analysis of the Trauma Audit and Research Network (TARN) database, an ongoing national study of trauma epidemiology in the United Kingdom. reported a significantly greater proportion of female patients (42%) in the geriatric group. This could be attributed to the demographic differences between the two regions and populations [10]. The geriatric age range as decided by the inclusion criteria in this study was found to be between 65-89 years and 18-27 years among the non-geriatric group. The mean age amongst this cohort was 72 and 39 years respectively and a similar mean age group of 75 years was reported [10]. Adults between the ages of 18-30 years in this study were found to be more prone to traumatic injuries due to their risk behavior which is common in young adults.
From the initial time of injury, the overall experience of an elderly person who sustains a traumatic injury can be very different from that of a younger patient with trauma, and special consideration should be given to proper triage and treatment of the geriatric patient with trauma. Once a geriatric patient arrives at a trauma centre, evaluation of the geriatric patient should proceed as is appropriate for their advancing age. Vital signs and physical examination can be deceptive in these patients, who may exhibit examination characteristics very different from those of younger patients. Although the ATLS protocol should be followed for geriatric patients just as it is for younger patients, there are some differences in the normal physiology of elderly patients that will make their evaluation and treatment more challenging. Elderly patients also subjectively report less pain for the same severity of injury than do their younger counterparts [11].
Certain vital parameters such as mean systolic blood pressure, mean pulse rate and GCS were recorded on admission in both the study populations, The geriatric population showed a much higher systolic blood pressure on admission at a mean of 130 mm of Hg across all the cases as compared to the non-geriatric age group which had a mean of 117 mm of Hg (Table 4). These observations suggest that the geriatric cardiovascular physiology who have higher baseline blood pressures and ejection fractions, lower left ventricular end-diastolic volumes, stroke volumes, and cardiac outputs compared to younger populations [12]. These findings in our study are in accordance with the findings of earlier reports where the geriatric trauma population also showed a higher mean systolic blood pressure, lower mean pulse rates as compared to the non-geriatric counterparts despite having a higher mean systolic blood pressure across all mechanisms of injury [13].
The physiology of aging affects every organ system in the geriatric person but the effects of this is most pronounced on the cardiovascular system and may significantly impact the care of the elderly trauma patient. These changes are mostly because of fundamental changes in the arteries that lead to decreased compliance, stiffness, and eventual hypertension [14]. The geriatric patients at baseline have systolic and diastolic dysfunction43 and a blunted response to adrenergic stimulation that may limit vasoconstriction42, 44 and the ability to mount a tachycardic response [15,16,17] which is frequently magnified by the chronic use of beta-blocking agents in this population. These physiologic changes also lead to cardiovascular comorbidities which are predominantly found in the elderly population as evidenced by the cardiovascular comorbidity rates found in the elderly in our study i.e. hypertension (50% vs 24%), ischaemic heart disease (13% vs 9%) and cerebrovascular disease (25% vs 17%).
Glasgow Coma Scale (GCS) scoring can be particularly difficult in the geriatric patient, who may have pre-existing cognitive deficits, hearing impairment, or other factors that can confound these examinations [18]. The clinical neurologic examination has also been shown to be unreliable in detecting significant hemorrhage in patients with minor head trauma [19]. Thus, a low threshold of reliability in ancillary studies on the geriatric patient with trauma has to be emphasized. In our study, the geriatric population had comparable rates of GCS
Several factors place the geriatric population at risk for traumatic events, and subsequent delayed recovery from trauma. Conditions that predispose patients to incur trauma are seen in higher prevalence in the elderly population. Weakness or chronic illnesses can lead to an increased rate of falls or other accidents in these patients. Loss of visual acuity, balance and gait instability, slowed reaction times, and cognitive impairments are also important disabilities that may lead to an increased incidence of traumatic events in the elderly. Often these issues are not recognized before the trauma, and cognitive dysfunction can be seen up to 35% of the time in the geriatric visitor to the emergency department but is only recognized 6% of the time [21]. Trauma itself is also an increased risk factor for future traumas, with elderly patients who have sustained trauma in the past being 3 times more likely to have a future traumatic event [21]. Owing to the constellation of problems seen in the elderly, prevention of geriatric trauma should be addressed by all clinicians caring for a geriatric patient.
Falls account for nearly three-quarters of all traumas in the geriatric population, with motor vehicle accidents accounting for nearly all the remaining 25% of injuries. Penetrating trauma and other mechanisms make up only 4% of total trauma in the geriatric population [22]. Among the elderly patients, nearly 90% experienced simple falls, such as falls from standing. Despite being simple mechanisms, the multiple comorbidities in the elderly population, along with the need for rehabilitation, make falls a significant medical and economic event in the life of these patients. Falls associated with blunt cerebral injury and long bone fractures lead to the greatest morbidity and mortality [23]. Ground level fall with head injuries coming in at (80%) and extremity injuries at (22%). With these injury patterns, it is not surprising that mortality was higher in geriatric patients after falls compared to the non-geriatric counterparts (25% vs 5%). Although ground level falls are a low-energy mechanism and may seem innocuous, mortality was higher in this series of geriatric patients (23% vs 0%). However, in the non-geriatric population, the most mechanism of injury was RTA (57%), with head injury (72%) followed by extremity injuries at 48%. Our findings are similar and comparable to ground level falls, mortality among older, aged patients reported elsewhere [24, 25]. In our study, deaths due to RTA in the geriatric group was 33% while RTA was the cause of death of 64.5% in the non-geriatric age group.
It should also be noted that 35% of the injuries that occurred secondary to RTA in the geriatric group were thoracic injuries. It has been well established that elderly patients with rib fractures are at increased risk for adverse outcomes including pneumonia, prolonged ICU stay and ventilator days, and increased mortality [26-28]. About one-quarter of all elderly victims of motor vehicle accidents sustain chest trauma, such as flail chest and rib fractures, which can complicate pre-existing cardiopulmonary disease and lead to pneumonia or respiratory failure, complications which are known to have particularly high morbidity and mortality [29,30]. RTA being high energy and velocity injuries contribute to much more varied and severe injuries in the elderly who have already compromised physiologies and thus, are unable to cope with the trauma.
Traumatic brain injury is quite common in geriatric patients after both falls and RTA and so, the trauma surgeon must realize the potentially lethal combination of TBI and older age. Geriatric trauma patients should receive liberal CT scanning for several reasons. With age comes brain atrophy that causes stretching of bridging veins and an increased risk of subdural hematoma [31]. Clinical decision-making tools commonly used to evaluate younger trauma patients should not be applied to older trauma patients [31]. Further, the neurological exam is unreliable in elderly patients and may miss significant TBI.
Injury Severity Score is an important method for describing patients with multiple injuries and evaluating emergency care. For a trauma centre intending to perform an effective review of their service, as well as for the scientific study of trauma, it is important to have an accurate benchmark of mortality risk. This benchmark serves as a predictor of mortality or "expected" outcome for any patient presenting with certain injuries. Trauma and Injury Severity Score (TRISS) utilizes the patient's age, type of injury, Revised Trauma Score (RTS), and the Injury Severity Score to estimate the probability of survival. It considers the patient's physiological injury, a physiological response and anatomic injury [32]. The Injury Severity Score (ISS), supplies the anatomic index for TRISS, and has been a standard tool for three decades. A major trauma (or polytrauma) is defined as the Injury Severity Score is greater than 15 [33,34]. In our study, both the geriatric and non-geriatric populations had comparable ISS>/=16 suggestive of major and severe trauma (252 vs 254). The geriatric trauma population had a higher crude mortality rate compared to the non-geriatric population even though both of them had similar ISS rates of 16 and above (39.3% vs 26.3%) which highlights that there are certain factors which are intrinsic to the geriatric group responsible for the higher mortality rate.
Co-morbidities are present in both the geriatric and non-geriatric populations but the relatively higher proportion of the various comorbidities in the geriatric population susceptible to the morbid nature of traumatic injuries. It is not uncommon to find multiple comorbidities in the geriatric population. Our study emphasized the fact that a large proportion of the geriatric population is hypertensive (50%), diabetic (27%). About 25% of them had sustained at least one episode of cerebrovascular accident, about 30% of them had diminished vision and 28% of them had diminished hearing respectively. These comorbidities have a significant impact on the response to a traumatic event in the geriatric population, who are already less healthy as compared to their younger counterparts. It is evident that the comorbidity profile in the geriatric age group is an important and independent risk factor for higher morbidity and mortality.
In our study, both the geriatric and non-geriatric trauma populations were subjected to operative interventions or otherwise afforded conservative management. About 45.3% of the geriatric population underwent various operative interventions while the rest of them were afforded conservative management. It should also be noted that the crude mortality rate of the geriatric age group is also higher compared to the non-geriatric population (39.3% vs 26.3%). Age is an independent risk factor for mortality in the geriatric age group and thus, a major operative intervention in the setting of an already compromised geriatric physiology with a superadded traumatic event is a major risk factor for mortality in such cases. Similarly, the majority of cases in the geriatric population were secondary to ground level falls leading to mainly head and extremity injuries as previously illustrated. It is interesting to note that the geriatric age group had a higher proportion of orthopedic and spinal surgeries as compared to craniotomies (22.8% vs 44.9%). A severe head injury is more life threatening is afforded priority in the case of a poly-trauma and thus, decides the line of management in such patients. It was observed that severe head injuries in the geriatric population (GCS
The non-geriatric population had a higher rate of undergoing operative interventions compared to the geriatric counterparts (56% vs 45.3%) with a crude mortality rate in the non-geriatric age group being 26.3%. This group had a higher percentage of Craniotomies and Laparotomies performed compared to the geriatric trauma population while the percentages of immediate lifesaving interventions like intercostal drain insertions were comparable in both groups. It is also noted that the geriatric trauma population group was afforded conservative management more commonly than operative interventional procedures. This could be attributed to the fact that a major operative intervention is a major risk factor for morbidity and mortality in geriatric trauma patients. An operative intervention has inherent risk factors including both surgical and anesthetic complications. However, it affects the geriatric population more than the non-geriatric population considering the already compromised physiology secondary to the process of aging.
In conclusion, elderly patients with trauma must be triaged, evaluated, and treated differently from their younger counterparts. Older adults have unique physiologic and structural differences that leave them at an increased risk of mortality even during minor trauma. Early recognition of these differences can lead to a better mortality rate and a more productive recovery after trauma along with the formulation of protocols specifically tailored for geriatric trauma patients.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
